By: Ethan Joyce

The Georgian government has struggled to facilitate adequate access to medical services for all of its residents. Looking at a map from the Georgia State Office of Rural Health reveals that 141 out of 159 counties in Georgia are currently designated as medically underserved, up from 130 counties a decade and a half prior.
The enduring repercussions of the COVID-19 pandemic, coupled with the state’s imbalanced adaptation to evolving federal funding, have further exacerbated disparities in access and quality of care. Together, these factors will actively shape Georgia’s capacity to achieve equitable healthcare provisions in the coming decades.
Background
In 2014, Governor Nathan Deal signed The Rural Hospital Stabilization Program into law, with the stated intention to create an oversight committee to evaluate recent hospital closures. The final recommendation of this committee was to create the Rural Hospital Stabilization (RHS) Grant Program in 2016. The grant program allows hospitals with increasingly tight margins to have more operational wiggle room, while simultaneously expanding access to primary care resources, reducing potentially preventable readmissions to decrease the overall burden on hospitals, and reducing inappropriate utilization of the Emergency Department.
While its impacts were significant, an initial report from phases one through three of the program demonstrated that only 67% of the original grant projects which began under the RHS grant program actually continued post funding. 15/18 implementers of the grant program said they would have either selected an entirely different program to fund, or would have made significant changes to the programs they funded using their grants. The report identified telehealth as the greatest grant program expenditure, while survey respondents identified telemedicine as the least beneficial or impactful project funded through the program.
In many respects the program has lived up to its expectations, allowing hospitals to develop rural infrastructure in accordance with local needs and desires while facing a multitude of external complications. However, comparing healthcare outcomes at the start of this program relative to healthcare outcomes today, we can observe its grave insufficiency in ameliorating the healthcare concerns of Georgians.
Recent Changes to State Funding
Recognizing that these programs did not meet the immediate needs of rural and impoverished communities, Georgia, in July, 2023, launched the Pathways to Coverage program. It imposed a work requirement for access to Medicaid coverage, with the idea that statewide funds would be used with increasing efficiency ending a reliance on what critics believe are handouts to low income individuals.
According to a GAO report from September, the results of the program are not promising. As recorded in April, Georgia spent $54 million on administrative costs since 2021, compared to only $26 million spent on health care costs. Additionally, the state projected enrollment of 25,000 individuals into Pathways in the first year while actual enrollment was approximately 4,300 individuals.
A GPBI report from October of 2025 states, “8,077 Georgians were actively enrolled in the Pathways to Coverage program by the end of the first two years, which represents no more than 7% of uninsured, low-income adults from working households.” Included in the same report was information relating to denial of coverage: authors cite concerns regarding a lengthy and burdensome paperwork process as the root cause for about 22% of application denials and about 30% of total program disenrollments. Ultimately the program has left the underlying issue of healthcare access unchanged, and the number of uninsured virtually unchanged as well.
Federal Adoption and Local Implications
Despite the program’s lackluster performance, GOP lawmakers have recently cited Georgia’s Medicaid work requirement as a paradigm of success, to be implemented at the federal level. The One Big Beautiful Bill Act (BBB), a budget reconciliation package signed into federal law on July 4 of this year, established work requirements that, while similar to Georgia’s, diverged in important respects. As a comprehensive legislative measure, the BBB also encompassed a range of provisions that affected healthcare access for Georgians across other dimensions.
Although Georgia recently rolled back certain reporting requirements for verifying monthly work status in response to the aforementioned GAO report released in September, the BBB reinstated the reporting policies that had previously proven difficult for the state to administer effectively. It remains uncertain whether state or federal legislation regarding reporting requirements will ultimately take precedence. So, in 2026 and 2027 when the BBB takes effect, conflicting reporting requirements could lead to increased expenditures related to healthcare administration instead of going toward the facilitation of healthcare services for Georgians.
Other key components of the BBB include the expiration of the Affordable Care Act (ACA) marketplace tax credit, which is now central to discourse surrounding the government shutdown, as well as the more than 1 trillion dollars in cuts to Medicaid. Georgians are already facing highly inflated premiums as a result. According to a report from the Center for Healthcare Quality and Payment Reform, nine of Georgia’s rural hospitals are at risk of closing within the year as a result of the expiry and austerity reforms (while there have been nine hospital closures in Georgia since 2010).
While some hospitals are facing complete closures, others will only close certain units, with obstetric medicine units facing some of the biggest cuts (they typically receive a higher percentage of Medicaid dollars and run with tighter operating margins). Recently, St. Mary’s Health Care System reported that their Heart Hospital in Lavonia would be eliminating their labor and delivery units, choosing instead to transfer OB-GYN patients to its facility in Athens. In a statement, they cited congressional funding changes in addition to some other structural challenges as direct causes for the closures.
Rural and low income patients are expected to be hit especially hard by this change, as experts suggest it will lead to increased transportation costs for individuals receiving care. Now, pregnant women will have to commute up to an hour and a half away to Athens or Gainesville to receive necessary treatments, a decision which could be life or death. While this is emblematic of a concerning trend, there was a component of the BBB which was put in place to address the adverse effects of the cuts to Medicaid on rural and low income populations. The Rural Health Transformation Fund (RHTF) is a 50 billion dollar federal rural health assistance program, where half of the program funds will be distributed equally across applicant states with the other half selectively apportioned according to the discretion of the Center for Medicare and Medicaid. While this program has the potential to temporarily insulate rural hospitals from the effects of the loss of Medicaid dollars, the total operating budget of the program pales in comparison to prior appropriations outlined for the Medicaid program. It is still yet to be seen whether or not this sum will prevent the degeneration of key state health infrastructure, as the program will last for only 5 years and Medicaid cuts are lasting.
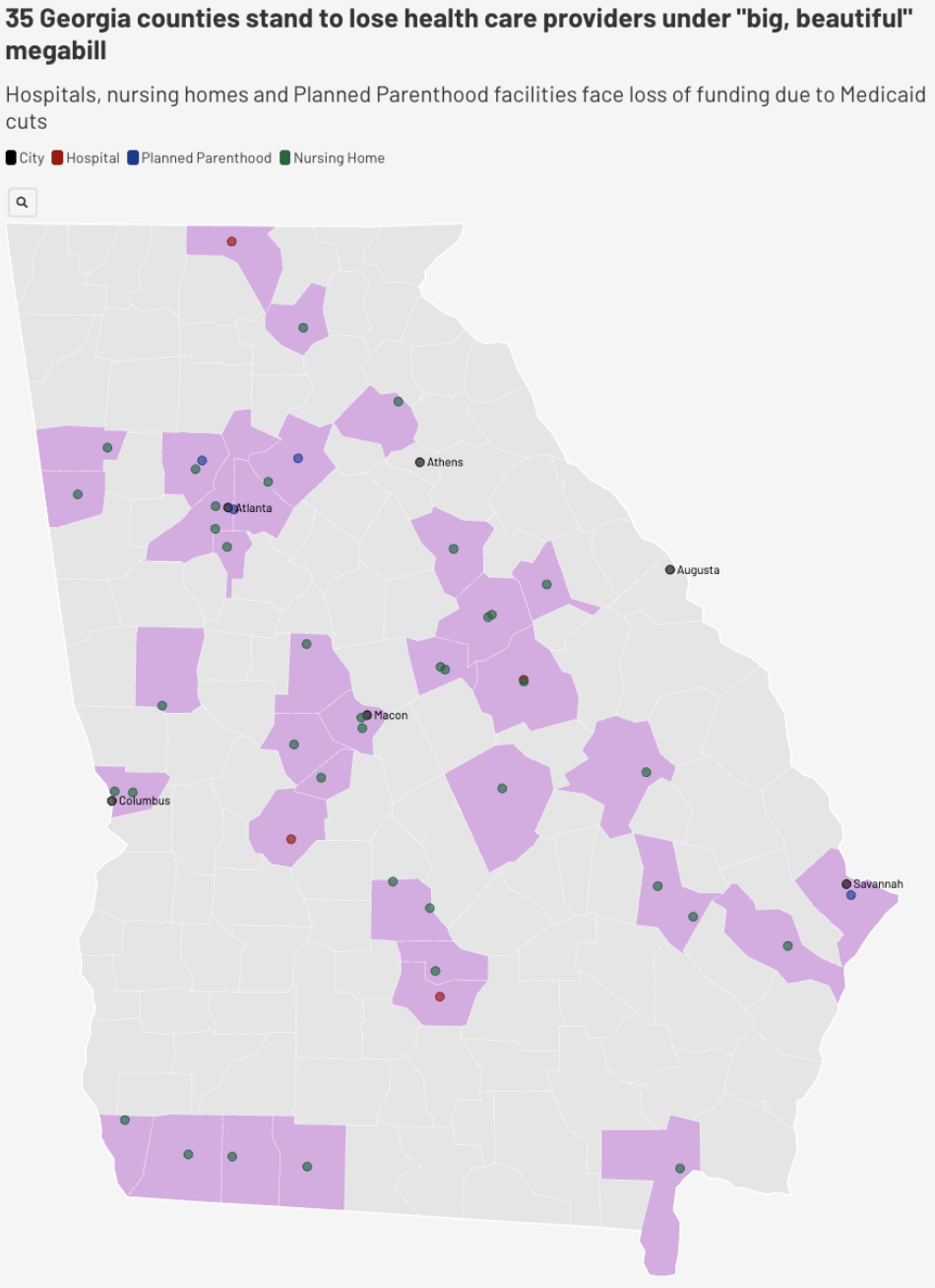
The latest data regarding provider coverage in Georgia, compiled by the Georgia Recorder, underscores how healthcare providers are steadily leaving the state, creating widening gaps in care access across rural and underserved regions. Projections indicate that without reform to the marketplace tax credit, more than 500,000 Georgians will lose insurance coverage on top of this reduction in general accessibility by January 2026.
With the expiration of pandemic-era federal funding injections and mounting fiscal pressures on essential services, these structural issues are becoming increasingly problematic. Many counties, particularly those without emergency hospitals, now face even more complex bureaucratic hurdles that threaten both service delivery and community health outcomes.
In this context, sustained advocacy for comprehensive healthcare reform is not simply advisable but imperative. Policymakers, healthcare leaders, and community stakeholders must work collaboratively to design solutions that stabilize provider availability, ensure equitable access to care, encourage new hires and doctor retention, and safeguard the health infrastructure upon which all Georgians depend. The future of healthcare in Georgia will depend on how decisively and inclusively these challenges are addressed moving into next year.

