By Madison Cruz
Ever since former president Richard Nixon coined the term “War on Drugs,” drug policy has been a hot topic for political debate. States like Colorado came to the forefront of news coverage with their recent legalization of marijuana, while other states like Alabama ensure that will never become their reality. Though the methods of attack are vastly different, all states can agree that something must be done about the drug epidemic in the country.
Differences in opinion on drug policy can usually be reduced to one fundamental disagreement: whether drug abuse is primarily a crime requiring punishment or an addiction requiring care and rehabilitation. Research and analysis of existing data indicate that drug policies that do not treat drugs as criminal behavior have produced more promising results. Solutions of that sort include access to mental health care, decriminalization of drugs, and solutions based in community or socialization.
Currently, in most states, any possession of a controlled substance is punishable by a minimum $1,000 fine and up to 1 year in prison. For years, drug abuse has been viewed as a criminal act. However, scientists have recently hypothesized that may not be the full story, instead proposing the self-medication theory.
Based on that hypothesis, providing personalized mental health care should theoretically be able to prevent dependency on illicit substances. Some argue providing this kind of care across the board is too lofty of an idea to be effectively put into practice, or that the costs would outweigh the benefits. Primary analysis for the effects of this change can be conducted, since certain states in the United States allot more funding to mental health care than others. If the theory stands, the states with good scores for mental health care access should conjointly have lower rates of arrests for illicit drug abuse, even when adjusted for third factors like poverty rates, education, etc.
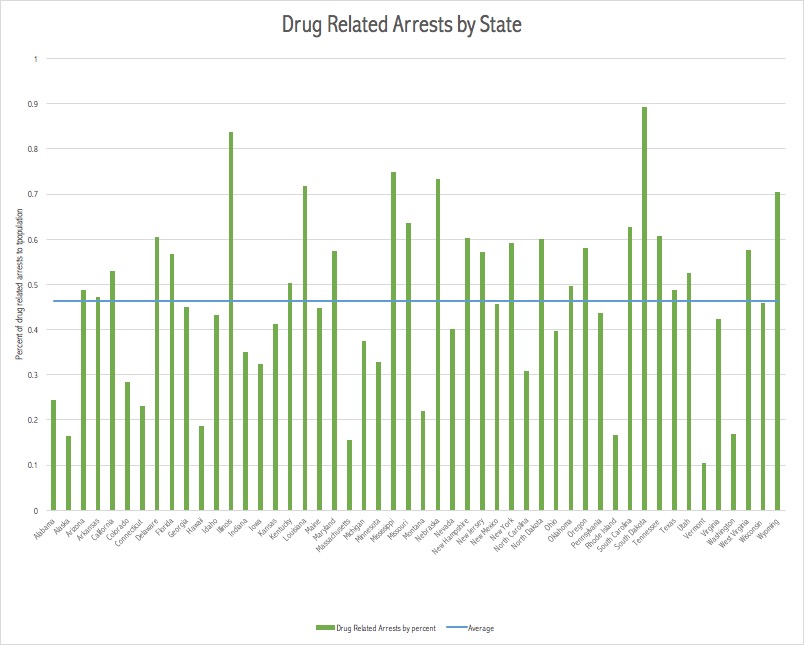
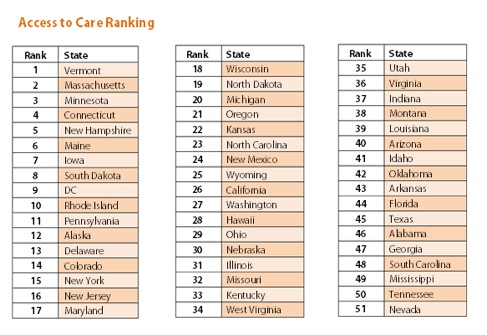
This correlation does stand, albeit loosely. In Figure 1 the rankings of states’ access to mental health care are represented, with the dark blue being the lowest ranked. The factors going into these rankings include “adults with disability who could not see a doctor due to costs,” “youth with MDE (major depressive episode) who did not receive mental health services,” among others. States like Vermont, Minnesota, and Massachusetts rate towards the top of that list. In the rankings of drug related arrests, displayed in Figure 2, those same states are ranked towards the bottom. In fact, Vermont in particular ranks #1 in mental health care access and #50 in drug related arrests. Massachusetts and Rhode Island also follow the same trend, ranking as the top mental health care providers and having the fewest drug related arrests.
Of course, the data isn’t perfect, with some significant outliers such as Illinois, which provides adequate mental health care but still ranks highly for drug related arrests. A large reason for the existence of these outliers is the prosecution of the War on Drugs through heavy policing of black communities. Thus, cities with larger black communities will have higher rates of arrests which do not necessarily correlate to higher rates of drug abuse. Despite these outliers, there is a sufficiently strong correlation between states’ investment in mental health care services and their citizens’ drug abuse tendencies to include discussion about mental health care access in drug policy debates.
Mental health care access is one rehabilitation based solution to the drug abuse problem, though decriminalization has also produced promising results in other countries. Portugal, for example, decriminalized illicit drug use in 2001, and researchers have since analyzed the effects of such a change. The data collected from 2001 until the present has shown that “among Portuguese adults, there are 3 drug overdose deaths for every 1,000,000 citizens. “Comparable numbers in other countries range from 10.2 per million in the Netherlands to 44.6 per million in the U.K., all the way up to 126.8 per million in Estonia. The E.U. average is 17.3 per million.”
In Portugal’s system, those found guilty of possession of small amounts of drugs are offered treatment from a psychologist, social worker, and legal adviser instead of jail time. This system is the most purely non-penal response to drug abuse, and for Portugal, it has been quite effective.
Portugal has a much smaller population than the United States and does not share its history of racially biased policing, so it is not a perfect model. However, the United States has an approach that contrasts starkly with Portugal’s, with arrests, imprisonment, and fines employed as commonplace techniques for disciplining those who abuse illicit substances. Considering the ineffective and inefficient nature of the United States’ current approach, it could perhaps stand to borrow some elements of more effective systems to create a stronger, more effective drug policy.
Researchers have also explored community and socialization as other possible care-focused solutions to drug abuse. Scientists in the late 1970s conducted an experiment demonstrating that crime-focused drug policy does not produce any productive change in treating and reorienting substance abusers into society; the experiment is often referred to as “Rat Park.” Scientists had previously set up a separate experiment with rats to prove how addiction works. It involved putting a rat in a cage with two water bottles: one with water, and one with water laced with opiates. Nearly every time, the rat would get addicted to the opiates and drink it until it died. This theory dominated scientific thought on addiction for years, until a group of colleagues at Simon Fraser University conducted a slightly different experiment. In their experiment, they put a rat in the same circumstances as previously observed as a control, a cage with the two water bottles, and observed the same result as before. However, they also set up what they called Rat Park: a rat utopia furnished with toys, other rats to socialize with, plenty of food and care, and the same two water bottles. In Rat Park, hardly any of the rats got addicted to the opiates: they would by chance drink it, but had no need to become addicted. They thus concluded that socialization and community play a bigger role in drug addiction than previously thought. Such a conclusion can be expanded to a societal model, with prison being the equivalent of the first rat’s circumstances. Focus needs to be shifted off of isolation and onto treatment and integration.
It is important to remember that oversimplification is dangerous, because human beings behave very differently than rats, and data can be skewed or misrepresented by confounding factors. But the Rat Park experiment, in conjunction with empirical data from the United States and countries that have decriminalized drug abuse, demonstrates that there is some merit in shifting our perspective away from the narrow crime-based drug viewpoint and further investigating if access to community and care can help reduce drug addiction, because the current system is simply not working. It is time to have productive dialogue about how public policy can most effectively end the “War on Drugs,” instead of trying to eradicate drug use by brute force, and that starts by identifying the core cause of the problem.